When gout flares up, it’s not just pain-it’s a sign your body is trying to tell you something deeper is wrong. The real problem isn’t the sudden joint swelling or the red, hot big toe. It’s the long-term buildup of uric acid crystals in your joints. And if you’re not treating that buildup, you’re just treating symptoms, not the disease. That’s why doctors now focus on one number: your serum urate level. The goal? Keep it below 6 mg/dL. For some, even lower-below 5 mg/dL. This isn’t guesswork. It’s science backed by decades of research and now built into global guidelines.
Why 6 mg/dL? The Science Behind the Target
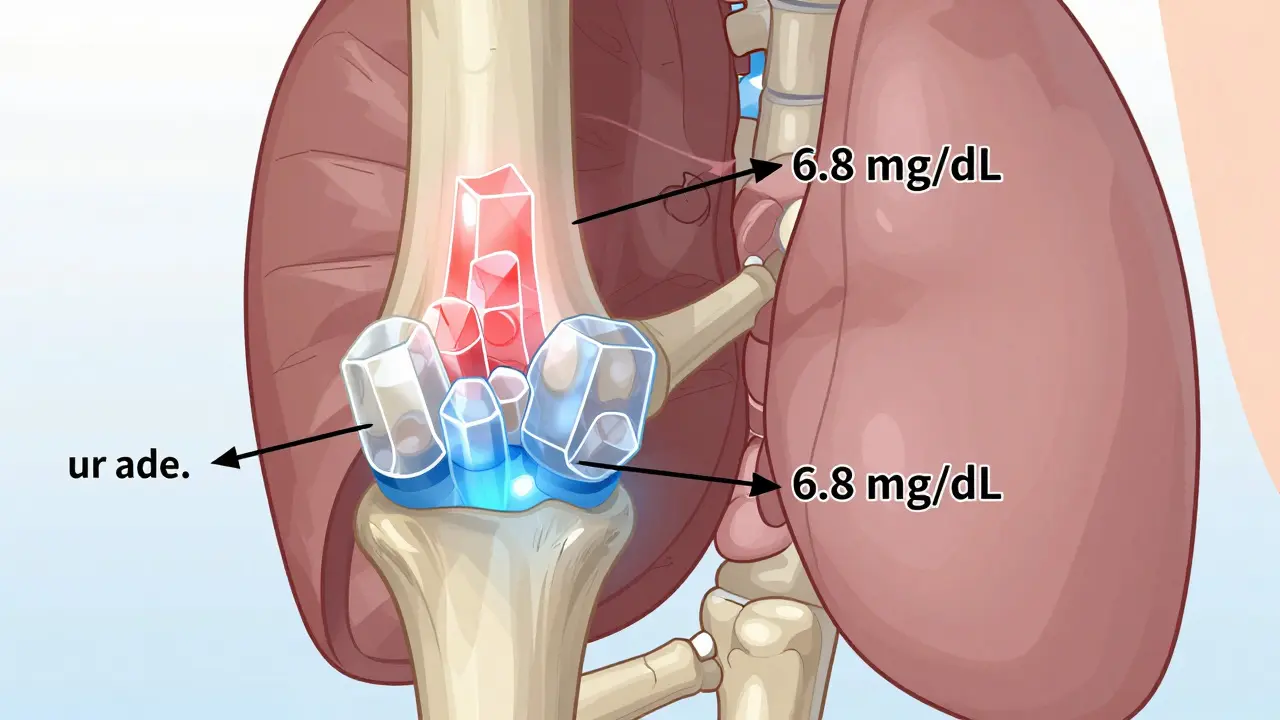
Uric acid dissolves in your blood up to a point. That point? About 6.8 mg/dL. Above that, crystals start forming. But here’s the catch: even if your level is just above 6 mg/dL, crystals can still grow slowly, damage joints, and cause flares. So the target isn’t to stay just under saturation-it’s to get well below it. That’s why major guidelines from the American College of Rheumatology (ACR), NICE, and EULAR all agree: 6 mg/dL is the minimum goal for most people with gout.
Why not go lower? Because there’s a sweet spot. Going below 3 mg/dL doesn’t help more-it might even cause problems. But if you have tophi (those visible lumps under the skin), joint damage seen on X-rays, or flares even while on treatment, you need to aim lower: 5 mg/dL. That’s not arbitrary. Studies show people who hit this lower target lose tophi faster and have 89% fewer crystal deposits over time.
The shift from "treat the flare" to "treat the urate" happened because of data. One study tracked 1,200 patients over five years. Those who kept their urate under 6 mg/dL had 74% fewer flares than those who didn’t. Another found that patients who stayed under 5 mg/dL saw their tophi shrink by half in just 18 months. This isn’t theory. It’s what happens in real people, in real time.
Allopurinol: The First-Line Workhorse
Allopurinol has been the go-to drug for gout since the 1960s. It works by blocking the enzyme that makes uric acid. Simple. Effective. Cheap. Generic allopurinol costs between $4 and $12 a month in the U.S. That’s why it’s still the first choice for most guidelines-even in patients with kidney disease.
But here’s the problem most doctors don’t tell you: most people start too low and never go higher. The standard starting dose? 100 mg a day. For many, that’s not enough. Studies show 30% to 50% of patients need doses over 300 mg/day. Some-even up to 600 or 800 mg/day-can reach target if their kidneys are working fine. The key? Titrate slowly, but don’t stop.
Start at 100 mg. Wait four weeks. Check your urate. If it’s still above 6 mg/dL, bump it up by 100 mg. Do this every month until you hit your target. Don’t wait three months. Don’t assume "it’ll work eventually." Most patients who never reach target do so because their dose was never increased. And yes, you can get your urate tested monthly. It’s not expensive. It’s critical.
There’s one big risk: allopurinol hypersensitivity syndrome. It’s rare-0.1% to 0.4% of users-but deadly. If you’re of Asian descent, especially Han Chinese, Korean, or Thai, you should get tested for HLA-B*5801 before starting. If you’re positive, don’t take allopurinol. Use febuxostat instead.
Febuxostat: The Alternative for Tough Cases
Febuxostat is newer, more expensive, and often misunderstood. It does the same thing as allopurinol-blocks uric acid production-but it’s processed differently. It doesn’t rely on kidney function as much. That makes it ideal for people with moderate to severe kidney disease.
A 2023 meta-analysis found febuxostat helped 15% more people reach their urate target than allopurinol in patients with CKD stage 3 or worse. That’s not small. It’s life-changing. For someone who can’t take allopurinol due to side effects, kidney issues, or genetics, febuxostat is a real option.
Start at 40 mg a day. Check urate after four weeks. If it’s still high, go to 80 mg. That’s it. No need to go higher. Most patients hit target at 80 mg. It’s not a "stronger" drug-it’s just better for certain bodies.
But here’s the catch: febuxostat isn’t for everyone. The FDA has a black box warning for heart-related death risk in people with existing heart disease. If you’ve had a heart attack, stroke, or unstable angina, avoid it. Stick with allopurinol. But if your kidneys are failing and you’ve tried allopurinol without success? Febuxostat might be your best shot.
The Treatment Gap: Why Most People Fail
Here’s the uncomfortable truth: only 42% of gout patients hit their urate target within a year. Why? It’s not the drugs. It’s the system.
- Doctors start patients on 100 mg of allopurinol and forget to follow up.
- Patients get scared when they flare more after starting treatment (yes, that happens-it’s called the "flare paradox").
- Testing urate levels is skipped because it’s "not covered" or "too much hassle."
Real-world data from New Zealand shows something shocking: Māori and Pacific patients are prescribed urate-lowering drugs more often-but they’re 23% less likely to reach target. Why? Longer wait times, language barriers, distrust in the system, and lack of culturally tailored education.
And then there’s the "I don’t feel pain, so I don’t need it" mindset. Gout isn’t about pain. It’s about crystals. You can have joint damage without a single flare. That’s why the ACR now says: if you have tophi or joint damage-even if you haven’t had a flare in two years-you still need treatment.
What Works in Real Life: Lessons from the Front Lines
Patients who succeed share three things:
- They test regularly. Monthly urate checks during titration boost success by 31%. If your doctor doesn’t offer this, ask for it.
- They dose up. The average successful patient takes 400 mg or more of allopurinol. If you’re on 300 mg and still flaring, ask: "Can I go higher?"
- They understand the flare paradox. When you start lowering urate, crystals start dissolving. That can trigger inflammation. It’s not a failure-it’s a sign the treatment is working. Ask for a short course of colchicine or NSAIDs during the first 6 months to prevent flares.
One patient I spoke with-61, diabetic, had tophi for 12 years-took 800 mg of allopurinol daily. She got her urate down to 4.8 mg/dL. Within a year, her tophi shrank by 70%. She still gets occasional flares-but they’re milder, shorter, and less frequent. She says: "I thought I was done with pain. Turns out, I was just getting started."
The Future: Precision and New Tools
Research is moving fast. The 2024 GOUT-PRO study showed that using genetic testing (for ABCG2 and SLC22A12 gene variants) to guide allopurinol dosing boosted target achievement from 61% to 83%. That’s huge. Imagine knowing your dose before you even start.
Next up? Drugs like verinurad-new uricosurics that help your kidneys flush out more uric acid. And trials like ULTRA-GOUT are comparing fixed doses versus titrated doses. Results are due by late 2025.
For now, the best tool is still simple: monitor, adjust, persist. Don’t settle for "it’s just gout." Gout is a metabolic disease. And like diabetes or high blood pressure, it responds to consistent, targeted treatment.
What to Do Next
If you have gout:
- Ask your doctor for a serum urate test-today.
- If it’s above 6 mg/dL, ask: "What’s my plan to get it down?"
- If you’re on allopurinol and still flaring, ask: "Can I go higher?"
- If you have kidney disease or a history of heart issues, ask: "Is febuxostat right for me?"
- Ask for colchicine or a short NSAID course for the first 6 months to prevent flares during treatment.
If you’re a caregiver or family member: help track doses. Remind them to get tested. Gout isn’t just a foot problem. It’s a whole-body disease. And it’s treatable-if you know how.
What is the ideal serum urate target for gout?
For most people with gout, the target is below 6 mg/dL (360 micromol/L). For those with tophi, joint damage, or frequent flares, the target drops to below 5 mg/dL (300 micromol/L). No one should aim below 3 mg/dL, as lower levels offer no extra benefit and may carry risks.
Why do I flare more after starting allopurinol or febuxostat?
This is called the "flare paradox." When urate levels drop fast, crystals start dissolving, which can trigger inflammation. It doesn’t mean the drug isn’t working-it means your body is reacting to the change. Most guidelines recommend taking colchicine or a low-dose NSAID for the first 6 months to prevent these flares.
Can I stop taking urate-lowering drugs once my urate is normal?
No. Gout is a chronic condition. Stopping treatment allows urate to rise again, and crystals will reform. Most patients need lifelong therapy. Even if you haven’t had a flare in years, your joints may still be damaged by crystals. The goal is to prevent future damage-not just stop pain.
Is febuxostat better than allopurinol?
It depends. Allopurinol is cheaper and works well for most people. Febuxostat is better for those with moderate to severe kidney disease or who can’t tolerate allopurinol. But if you have heart disease, febuxostat may increase risk. Always discuss your full medical history with your doctor before choosing.
How often should I get my urate level checked?
When starting or adjusting dose, check every 4 to 6 weeks. Once you hit your target and stay there for 6 months, you can space it out to every 6 months. But don’t skip it. Urate levels can creep up without symptoms. Regular testing is the only way to know if your treatment is working.
Can I manage gout with diet alone?
Diet helps, but it’s not enough. Even the strictest low-purine diet lowers urate by only 1 to 2 mg/dL. Most people need medication to reach the target of 6 mg/dL or lower. Diet should be part of your plan-not the whole plan.


10 Comments
peter vencken
I've been on allopurinol for 5 years and honestly? The only reason I stuck with it is because my doc kept pushing me to titrate. I started at 100mg like everyone does. Flared like crazy. Thought it was broken. Then she said 'go to 200'... then 300... then 400. At 400mg my urate hit 5.2. No more tophi. No more midnight pain. It's not magic. It's math. And most docs don't do the math.
Also diet? Nah. I still eat steak. Just take my pill.
Aaron Sims
So... let me get this straight. You're telling me the entire medical industry is just now figuring out that crystals = bad? And we've been giving people painkillers for 50 years while their joints turned to dust? And now we're supposed to believe this '6 mg/dL' thing is science? Bro. That's the same number they used for 'safe' lead levels in kids in the 80s. I'm suspicious.
Darlene Gomez
This is one of the clearest, most evidence-based explanations of gout management I've ever read. Thank you for laying out the titration protocol so plainly. So many patients are abandoned after the first flare. The fact that we're still not routinely checking urate levels monthly during titration is a systemic failure. I'm a nurse practitioner and I'm implementing this exact protocol in my clinic next week. Let's stop treating gout like it's a nuisance and start treating it like the metabolic disease it is.
Rama Rish
As someone from India, I see so many patients with gout who think it's just 'hot food' problem. They stop meds when pain goes away. But the crystals? They don't care. They just keep building. I tell them: your joint is not a trash can. You can't just throw away the trash once it's full. You gotta clean it out slowly. Allopurinol is the broom. Not the napkin.
Korn Deno
The real revolution isn't the drug. It's the shift from symptom management to disease modification. We do this with hypertension. With diabetes. Why is gout still treated like a one-time party crasher? It's not. It's a slow-motion autoimmune-metabolic cascade. And we're finally learning to intervene before the damage is irreversible. That's huge. We're not just preventing pain. We're preventing disability.
Katie Putbrese
I don't trust these newfangled meds. Allopurinol's been around since Nixon. Why switch? Febuxostat? Sounds like a drug company scam to sell expensive pills. And why do we need to test blood every month? My uncle took pills for 20 years and never checked anything. He's fine. Maybe we're overmedicating because we're scared of lawsuits.
Amber Gray
I've been on 600mg allopurinol for 3 years. Urate at 4.9. No flares. No tophi. Just a little weird numbness in my toes sometimes. But I'll take it. Also I use emojis now because why not 😎💊📉
Jacob Hessler
My doc said go to 800mg. I said no way. Too much. Then I read this. Did it. Urate down. Tophi shrinking. Now I'm telling everyone. Stop being scared. Just take the damn pill. And yes I misspelled 'damn'.
Danielle Arnold
I read the whole thing. Then I went to my doctor. She said 'just take colchicine when it flares.' I said 'but the article says...' She sighed and handed me a $5 coupon for ibuprofen. So yeah. I'm still flaring. But at least my wallet's happy.
Kevin Y.
I appreciate the depth of this post. As a physician who has managed gout patients for over a decade, I can confirm that the most common failure point is not pharmacology-it's adherence to titration protocols. We must normalize monthly urate monitoring. It is not burdensome. It is essential. I have personally seen patients regain mobility after 15 years of disability simply by achieving sustained urate targets. This is not theoretical. It is transformative. Thank you for highlighting the data.