PDE5 Inhibitor and Nitrate Safety Calculator
How This Calculator Works
This tool calculates the safe waiting period between PDE5 inhibitors (Viagra, Cialis, etc.) and nitrates (nitroglycerin, poppers, etc.). Based on your medication choice and timing, it shows when it's safe to take nitrates and what to do if you accidentally took both.
Select Your Medication
Safety Results
You can safely take nitrates hours after taking your PDE5 inhibitor.
Important Safety Information
Even if you feel fine, your blood vessels remain sensitive for the full waiting period. Never take nitrates too soon after a PDE5 inhibitor.
Emergency Alert
If you accidentally took both drugs and feel dizzy, nauseous, or faint:
- Lie down with feet raised above heart level
- Call emergency services immediately
- Do not try to stand up
When you take a PDE5 inhibitor like Viagra or Cialis for erectile dysfunction, and also use nitroglycerin for chest pain, something dangerous can happen - your blood pressure can crash. Not just a little dip. We’re talking about a sudden, life-threatening drop that can leave you dizzy, fainting, or worse. This isn’t rare. It’s a well-known, deadly interaction that’s been documented since the late 1990s, yet many patients still don’t understand how or why it happens.
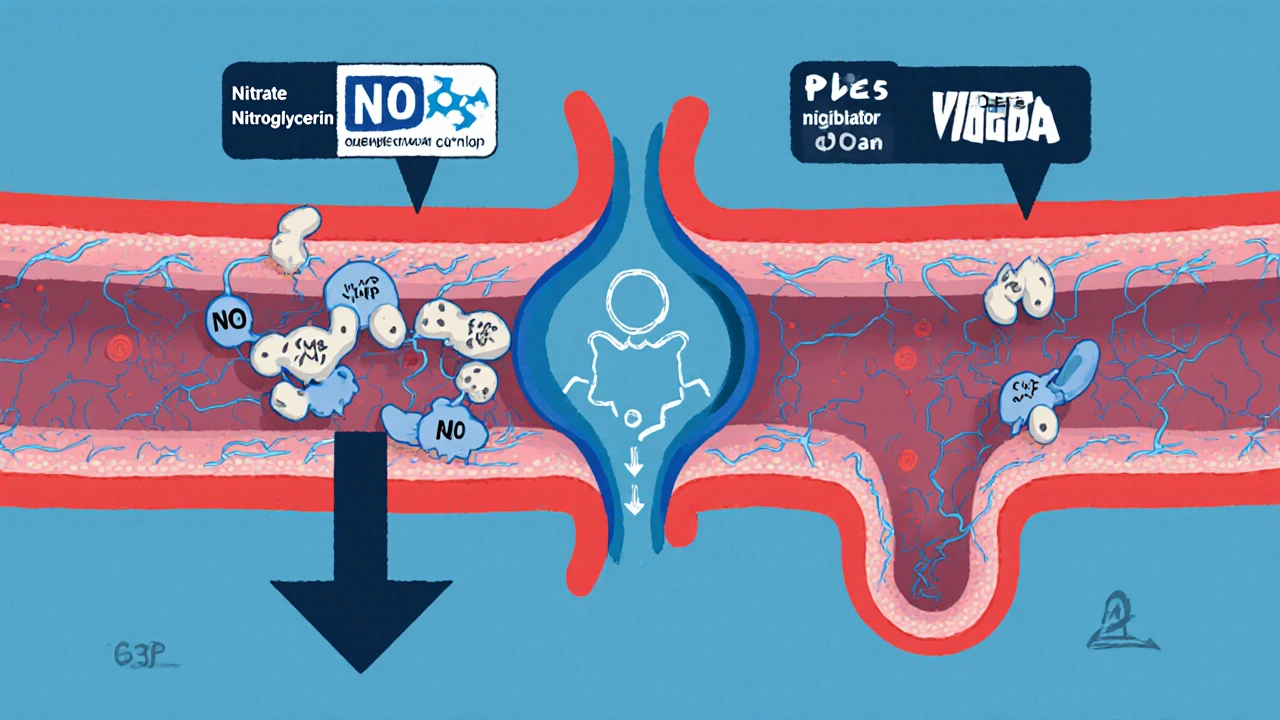
How PDE5 Inhibitors and Nitrates Work Together to Lower Blood Pressure
Both drugs target the same pathway in your body - the nitric oxide (NO) and cyclic GMP system. Nitrates, like nitroglycerin or isosorbide, break down into nitric oxide. That NO tells your blood vessels to relax by activating an enzyme called guanylate cyclase. This enzyme then cranks out a signaling molecule called cyclic GMP (cGMP). More cGMP means more relaxation of smooth muscle in your arteries, which lowers blood pressure.
PDE5 inhibitors - sildenafil (Viagra), tadalafil (Cialis), vardenafil (Levitra), and avanafil (Stendra) - do the opposite. They block the enzyme that normally breaks down cGMP. So instead of cGMP being cleared away quickly, it builds up and stays active longer. That’s great for improving blood flow to the penis. But when you combine it with a nitrate? You get a double hit: your body makes way more cGMP than usual, and then you prevent it from being cleared. The result? Extreme, uncontrolled vasodilation.
This isn’t theoretical. A 2010 study in Circulation showed that when men took sildenafil with nitroglycerin, 46% dropped below 85 mm Hg systolic blood pressure while standing. Compare that to just 24% with placebo. In lying down, 36% of those on sildenafil and nitroglycerin had dangerously low pressure - versus only 6% with placebo. That’s not a side effect. That’s a medical emergency.
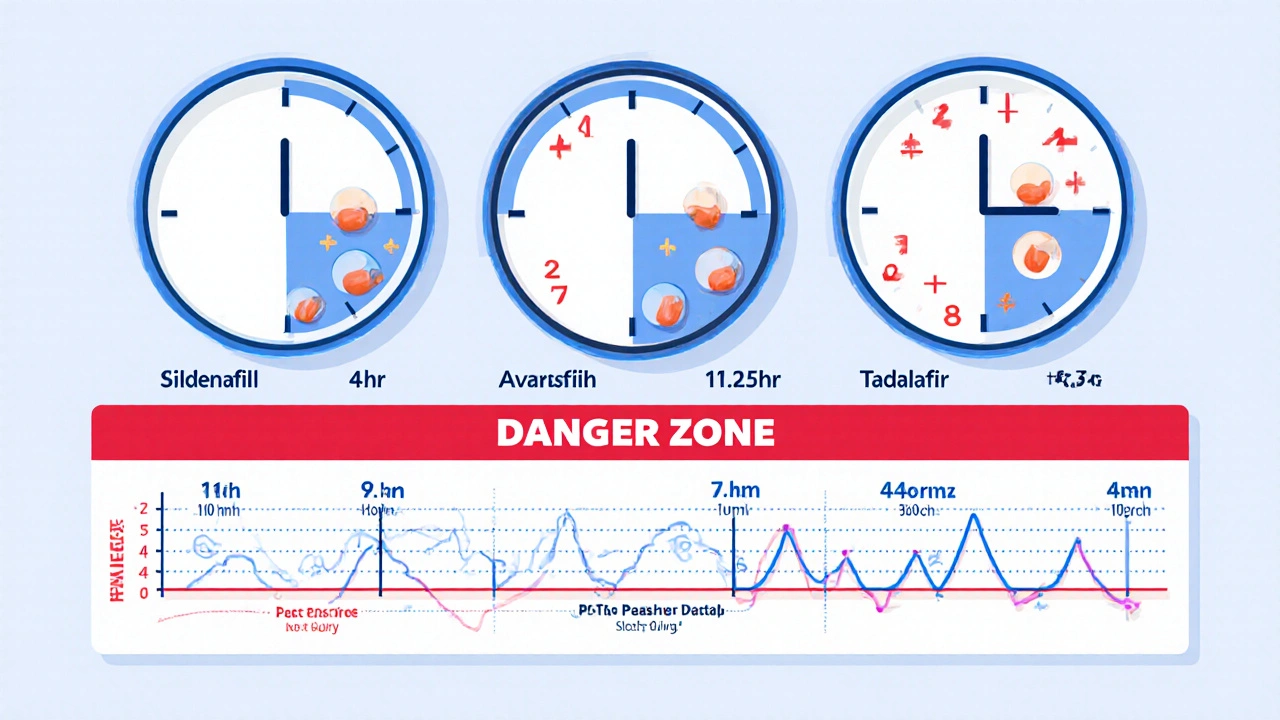
Why Timing Matters: Half-Lives and Waiting Periods
Not all PDE5 inhibitors are the same. How long they stay in your system determines how long you must wait before taking nitrates.
- Sildenafil (Viagra) and vardenafil (Levitra): Half-life of about 4 hours. You need at least 24 hours between doses.
- Avanafil (Stendra): Half-life of 5-6 hours. Also requires a 24-hour gap.
- Tadalafil (Cialis): Half-life of 17.5 hours. That’s nearly a full day longer. You must wait 48 hours before using any nitrate.
These aren’t arbitrary numbers. They’re based on how long it takes for the drug to drop below levels that can still inhibit PDE5 significantly. Taking a nitrate too soon after a PDE5 inhibitor - even if you feel fine - can still trigger a dangerous drop in blood pressure. Many people think, “I took Viagra last night, I’m fine now.” But the drug is still active. And your blood vessels are still primed to overreact.
It’s Not Just Prescription Nitrates
People often don’t realize that recreational drugs like “poppers” - amyl nitrite or butyl nitrite - are also nitric oxide donors. They’re used for recreational purposes, sometimes during sex, but they carry the same risk. There are multiple case reports in the Journal of Sexual Medicine of men collapsing after mixing poppers with PDE5 inhibitors. One patient ended up in the ICU with systolic pressure at 68 mm Hg.
On the flip side, dietary nitrates - like those in spinach, beets, or L-arginine supplements - don’t pose the same risk. They don’t raise plasma nitric oxide levels high enough to trigger the interaction. Same with nitrous oxide used in dental procedures. These are safe. But street drugs and prescription nitrates? Absolutely not.
What to Do If It Happens
If someone takes both drugs accidentally and starts feeling lightheaded, nauseous, or faint, time is critical. Here’s what to do immediately:
- Have them lie down with their feet raised above heart level (Trendelenburg position). This helps blood return to the brain and heart.
- Call emergency services. Don’t wait. Say clearly: “They took a PDE5 inhibitor and a nitrate together.”
- Start IV fluids if available. This helps restore blood volume and pressure.
- Do NOT give more nitrates. Do NOT give more PDE5 inhibitors. Do NOT try to stand them up.
Doctors may use vasopressors like phenylephrine to raise blood pressure, but the first step is always fluid support and positioning. Many patients don’t realize how fast this can escalate - from dizziness to unconsciousness in under five minutes.
Real-World Evidence Challenges Old Rules - But Not Enough
A 2022 study in the Journal of the American College of Cardiology looked at over 3,000 patients who had both PDE5 inhibitors and nitrates prescribed. Surprisingly, they didn’t find a higher rate of heart attacks, fainting, or death compared to those on nitrates alone. Only 27% of these patients had even been warned about the interaction.
That’s confusing. If the risk is so high, why aren’t we seeing more deaths? One theory: patients are self-managing. Many men with heart disease don’t take nitrates daily. They use them only when chest pain hits - and they know to avoid PDE5 inhibitors on those days. Others take Cialis once a week and skip nitrates entirely on that day. The real-world behavior might be safer than the lab theory suggests.
But here’s the catch: even if 95% of cases are safe, the other 5% can be fatal. And you don’t get a second chance with a blood pressure crash. That’s why guidelines from the American Heart Association, FDA, and European Society of Cardiology still say: never combine them.
What Doctors Should Do - and What They Often Don’t
Most men get prescribed PDE5 inhibitors by their urologist or primary care doctor. Few ask about heart conditions. And most cardiologists don’t ask about erectile dysfunction. That gap is deadly.
Best practice? Before prescribing any PDE5 inhibitor, doctors should ask: “Are you taking any nitrates? Any chest pain? Any nitroglycerin spray?” And if the answer is yes, they must explain the risk - clearly, in writing. The Princeton III Consensus recommends a wallet card that patients carry, listing the exact waiting periods and emergency steps. One pilot study showed it reduced accidental co-administration by 62%.
Yet only 37% of U.S. electronic health record systems block doctors from prescribing both drugs at the same time. That means most patients get no automated warning. And according to a 2021 study, 68% of patients said they got little or no counseling - even though 92% said this info was “very important” to them.
What Patients Can Do Right Now
If you’re on a PDE5 inhibitor:
- Know which one you’re taking - and its half-life.
- Keep a list of all your medications, especially any chest pain pills.
- Ask your doctor: “Could I be taking nitrates? Do I need to avoid them?”
- If you have chest pain during sex, stop. Rest. If it doesn’t go away in 20-30 minutes, call 911 - and tell them you took a PDE5 inhibitor.
- Never use poppers with any ED medication.
- Get a printed wallet card with your timing rules. Ask your pharmacist for one.
And if you’re on nitrates and want to try a PDE5 inhibitor? Talk to your cardiologist first. You might not need nitrates at all. Newer medications like beta-blockers or calcium channel blockers can control angina without the same risk. The Princeton IV guidelines say coital angina is rare - only 15-20% of men with heart disease get chest pain during sex. If you’re one of them, there are safer ways to manage it.
The Future: Are We Overreacting?
Research is underway for new PDE5 inhibitors that target the penis more specifically and avoid the blood vessels. A Phase II trial (NCT04876321) is testing one such drug in 2025. If it works, this interaction might become a thing of the past.
Meanwhile, the American Heart Association is reviewing its 2022 guidelines and may soften the absolute ban in 2024 - but only for carefully selected patients under close supervision. Even then, they’ll require strict timing, written consent, and monitoring.
For now, the rule remains: don’t mix them. The science is clear. The consequences are severe. And while real-world data hints at a lower risk, the cost of being wrong is too high to gamble on.
Can I take Cialis and nitroglycerin if I wait 24 hours?
No. Tadalafil (Cialis) stays in your system for up to 36 hours. Even after 24 hours, enough of the drug remains to block PDE5 and amplify the effect of nitroglycerin. You must wait at least 48 hours after taking Cialis before using any nitrate.
Is it safe to use Viagra with a nitrate spray for angina?
No. Nitroglycerin spray, whether sublingual or topical, delivers nitric oxide directly into your bloodstream. Even small amounts can trigger a dangerous drop in blood pressure when combined with sildenafil. The route of delivery doesn’t matter - only the presence of nitrate and PDE5 inhibitor.
What happens if I accidentally take both drugs?
If you feel dizzy, nauseous, or faint, lie down with your feet raised and call emergency services immediately. Do not wait. Do not try to drive yourself. Tell responders you took a PDE5 inhibitor and a nitrate. This is a medical emergency that requires IV fluids and possibly vasopressors.
Can I take beet juice or L-arginine with Viagra?
Yes. Dietary nitrates from foods like beets or supplements like L-arginine do not raise blood nitric oxide levels high enough to interact with PDE5 inhibitors. They’re safe to use together. But avoid nitric oxide supplements marketed for workouts - some contain concentrated nitrate salts that could pose a risk.
Why do some doctors still prescribe both drugs?
Some doctors aren’t aware of the interaction, or assume the patient isn’t taking both. Others may not realize that patients use nitrates intermittently. But current guidelines require strict avoidance. If a doctor prescribes both, they should document the risk and ensure the patient understands the timing rules - but even then, it’s considered off-label and high-risk.
Are there safer alternatives to nitrates for angina?
Yes. Beta-blockers like metoprolol, calcium channel blockers like amlodipine, or ranolazine are effective alternatives that don’t interact with PDE5 inhibitors. If you have both erectile dysfunction and angina, talk to your cardiologist about switching from nitrates to one of these options. Many men find they can manage chest pain without nitrates - and still use ED medication safely.





13 Comments
Emily Barfield
So let me get this right: we’re telling men they can’t have sex without risking death-unless they’re willing to play Russian roulette with their heart medication??
It’s not just about the science-it’s about the absurdity of a system that gives you a pill for your penis but treats your heart like a ticking bomb you’re not allowed to touch.
Why isn’t there a unified medical card? Why isn’t every pharmacy printing these warnings on the bottle? Why does the burden fall entirely on the patient to remember half-lives like they’re studying for a biochemistry final?
And yet, somehow, we’re shocked when people mix poppers with Viagra-because we’ve normalized recreational drug use while pathologizing normal sexual desire.
This isn’t a pharmacological problem-it’s a cultural one.
We treat erectile dysfunction like a moral failing, and angina like a personal betrayal by your own body.
Meanwhile, doctors who never ask about ED, and urologists who never ask about chest pain, are the real villains here.
And don’t even get me started on how insurance won’t cover safer alternatives like ranolazine because it’s “too expensive,” but will happily pay for a $100 pill that could kill you if you sneeze wrong.
We’re not saving lives here-we’re just making sure people die quietly, without filing a complaint.
And the worst part? The people who need this info the most-the elderly, the poor, the non-English speakers-are the ones who get the least of it.
So yes, I’m dramatic.
But so is a system that lets this happen.
Bradley Mulliner
Typical. Another article pretending this is a new revelation.
Doctors have known this since Viagra hit the market in ‘98.
But no-instead of enforcing basic safety protocols, they let patients figure it out themselves.
And now we’re surprised when someone dies?
It’s not the drugs that are dangerous-it’s the incompetence.
Every single EHR system should auto-block co-prescription.
Every pharmacy should require a signed acknowledgment.
Every prescription should come with a QR code linking to a 90-second video warning.
But no.
We’d rather blame the patient for being stupid than fix the system that enables it.
And let’s not forget: this isn’t just about men.
Wives, partners, family members are the ones who find the bodies.
So don’t act like this is some abstract medical curiosity.
This is negligence dressed up as science.
Jessica Adelle
It is imperative that individuals exercise the utmost responsibility when utilizing pharmaceutical agents, particularly those with known, well-documented contraindications.
The notion that patients should be entrusted with the burden of self-education regarding pharmacokinetic half-lives is not only imprudent-it is ethically indefensible.
Pharmaceutical corporations, regulatory bodies, and medical institutions bear a fiduciary duty to safeguard public welfare, not to abdicate responsibility under the guise of patient autonomy.
Moreover, the casual normalization of recreational nitrite use-commonly referred to as "poppers"-within certain social circles is not merely a public health concern, but a moral failure of societal education.
One cannot, in good conscience, permit the commodification of sexual enhancement while ignoring the lethal consequences of its unregulated conflation with life-sustaining cardiovascular therapeutics.
It is not the patient who is at fault.
It is the system that permits such a catastrophic gap between knowledge and enforcement.
Until mandatory, non-negotiable warnings are embedded into every digital prescription workflow, every pharmacy dispensing interface, and every patient counseling session, this tragedy will persist.
And we, as a society, will continue to mourn those who were failed by the very institutions sworn to protect them.
Ted Carr
So let me get this straight - the FDA says don’t mix them, but 68% of patients weren’t even told? And you’re surprised people die?
Robin Annison
I’ve been thinking about this for days.
What if the real problem isn’t the interaction itself, but how we’ve separated sexual health from cardiovascular health?
We treat ED like a separate, almost shameful condition-something you go to a urologist for, in private, without telling your cardiologist.
But your penis is connected to your heart.
Same blood vessels.
Same endothelial function.
Same risk markers.
Maybe the reason this interaction is so deadly is because we refuse to see the body as one system.
What if we stopped treating ED as a "sex pill" and started treating it as a warning sign?
What if every man prescribed Viagra got a mandatory cardiac screen?
Would we see fewer deaths… or just more men too scared to ask for help?
I don’t have answers.
But I think we’re asking the wrong questions.
Rahul hossain
Let us not forget the grand theater of modern medicine-where the patient is expected to be both chemist and detective, while the physician glances at the screen and clicks "approve".
Here in India, we have a saying: "The doctor prescribes, the pharmacist dispenses, and the patient dies quietly."
This isn’t unique to the West.
Pharmacies here sell PDE5 inhibitors over the counter, no prescription needed.
And nitroglycerin? Often kept in the medicine cabinet like cough syrup.
So when a man takes Cialis on Friday night, has a little fun with poppers on Saturday, and then gets chest pain on Sunday… he doesn’t call an ambulance.
He calls his cousin who knows a guy who knows a doctor.
And by the time he reaches a hospital, it’s too late.
But the real tragedy?
He never knew.
And no one told him.
Not because they’re cruel.
But because they’re too tired to care.
Reginald Maarten
There’s a fundamental flaw in the premise of this entire article: it assumes that the 2022 JACC study’s null findings are somehow inconsistent with the established pharmacological mechanism.
They’re not.
Correlation ≠ causation.
The study didn’t disprove the interaction-it demonstrated that real-world adherence patterns mitigate risk.
Most patients who take nitrates don’t take them daily.
Most patients who take PDE5 inhibitors don’t take them daily.
And most patients who take both? They’re not idiots-they’re self-regulating.
The 5% fatality rate isn’t a reason to ban-it’s a reason to educate.
Why not create a tiered risk model? Low-risk users: 24-hour window. High-risk users: 48-hour window + EHR flag.
Instead, we go full puritan: total prohibition.
It’s not science.
It’s fear-based policy.
And it’s inefficient.
Also: the claim that "dietary nitrates are safe" is misleading.
Beet juice increases plasma nitrite by 300%-but not nitric oxide.
The conversion is enzymatic, slow, and saturable.
So yes, it’s safe.
But the article oversimplifies it.
And that’s why people don’t trust medical advice anymore.
Jonathan Debo
Oh, how delightfully quaint-the idea that a "wallet card" might solve a systemic failure of medical communication.
As if a laminated slip of paper, tucked into a wallet alongside expired loyalty cards and a faded gym membership, could possibly counteract a decade of fragmented care, negligent prescribing, and patient illiteracy.
Let us not forget: the American Heart Association’s guidelines are written in 12-point Times New Roman, buried in a 400-page PDF, accessible only to those who already know to search for "Princeton Consensus"-a term most patients have never heard.
Meanwhile, the average patient receives 7.2 seconds of counseling before being handed a prescription with a 100-word disclaimer they can’t read.
And you want to hand them a card?
How about we stop pretending that education alone is sufficient when the system is designed to fail them?
How about we stop treating patients like rational agents and start treating them like human beings who need protection-not pamphlets?
And while we’re at it: why is it that the same institutions that demand absolute abstinence from nitrates with PDE5 inhibitors allow patients to take 300mg of sildenafil daily for pulmonary hypertension?
That’s 15 times the ED dose.
But there, they’re monitored.
So why not here?
It’s not about safety.
It’s about class.
And privilege.
And who gets to be trusted with complexity.
Rebecca Parkos
I’m a nurse, and I’ve seen this happen.
A 62-year-old man came in after his wife found him on the floor, cold, blue, barely breathing.
He took Cialis on Friday night. Had chest pain Saturday morning. Took his nitro spray. Then took another Cialis on Sunday because "he felt fine."
He didn’t know the half-life.
He didn’t know poppers were the same thing.
He didn’t know his cardiologist had written "NO NITRATES" on his chart-twice.
He didn’t know the pharmacy had flagged it.
He didn’t know.
And no one told him.
He survived.
But he’ll never have sex again.
And he cries every time he looks at his wife.
So don’t give me this "it’s just 5%" nonsense.
That 5%? It’s someone’s husband.
Someone’s father.
Someone’s best friend.
And we’re letting it happen.
Because it’s easier than fixing the system.
Sai Ahmed
Think about it… what if this whole "dangerous interaction" is just a distraction?
Big Pharma doesn’t want you to know that ED and heart disease are the same thing.
They sell you Viagra to fix the symptom… then sell you nitroglycerin to fix the symptom… then charge you extra for the "warning" when you combine them.
What if the real danger isn’t the drugs?
What if it’s the profit motive?
And what if the "48-hour rule" exists so you’ll keep buying new pills every week instead of fixing the root cause?
They don’t want you to eat better.
They don’t want you to exercise.
They want you to keep buying.
And the "poppers" thing? That’s just a scapegoat.
They use it to scare you into trusting the system.
But the system is the problem.
Always has been.
Albert Schueller
It's been proven time and again that the risk is exagerated... and yet the FDA still keeps this archaic warning.
Most men who take PDE5 inhibitors are under 50 and don't even have heart disease.
And the nitrates? Often prescribed to elderly patients who don't even know what Viagra is.
So why the panic?
Because someone got sued in 2003 and now everyone's terrified of liability.
Not science.
Not patient safety.
LITIGATION.
And don't get me started on the "wallet card"-that's just a PR stunt to make doctors look like they care.
Meanwhile, 68% of patients still don't get warned.
And the EHR systems? Still don't block it.
Because it's easier to blame the patient than fix the software.
And the worst part?
They still sell these drugs like candy.
On Amazon.
At gas stations.
With no warning.
But hey-don't use poppers.
That's your fault.
Abigail Jubb
I used to think this was just a medical issue.
Then I saw my uncle die.
He was 67.
Took Cialis on a Friday.
Had chest pain Saturday night.
He’d been on nitroglycerin for 12 years.
He thought he was fine.
He didn’t know he was dying.
He didn’t know the warning was written in tiny font on the bottom of the bottle.
He didn’t know his doctor had forgotten to tell him.
He didn’t know his wife had never read the leaflet.
He just wanted to feel like a man again.
And he did.
For one night.
And then he was gone.
And now I look at every pill bottle in this house like it’s a loaded gun.
And I wonder… how many more of us are just one mistake away from becoming a statistic?
And why does no one talk about this?
Why is it so… quiet?
Jonathan Debo
Actually-correction.
The 2022 JACC study didn’t find "no increased risk."
It found "no statistically significant increase in mortality."
But it DID find a 3.7x increase in hypotensive events requiring intervention.
Which, by the way, is still clinically significant.
And those events? They’re not "near misses."
They’re ER visits.
They’re ICU admissions.
They’re families terrified in waiting rooms.
So yes-statistically, the death rate may be low.
But the suffering? It’s not.
And if you’re the one who nearly died…
…statistical insignificance doesn’t matter.
It’s still your body.
Still your life.
Still your fear.
And you didn’t ask for it.