
When a pharmacist fills a prescription for a controlled substance, they’re not just handing out pills-they’re stopping a potential overdose, a diversion, or even a death. One wrong number, one unclear direction, one unverified DEA number, and the whole system cracks. The stakes aren’t theoretical. In 2022 alone, controlled substance verification failures led to over 6,200 enforcement actions by the DEA against pharmacies and prescribers. That’s not a statistic-it’s a warning.
What Exactly Must Be Verified?
Every controlled substance prescription must pass seven checks before it’s dispensed. Missing one means the prescription is invalid, no matter how legitimate it looks. These aren’t suggestions. They’re federal law under 21 CFR § 1306.05.- Prescriber’s full name and address - Must match the DEA registration exactly. No abbreviations. No PO boxes unless explicitly allowed.
- Date of issuance - For Schedule II drugs, the date must be today. For Schedules III-V, it must be within the last six months.
- Patient’s full name and address - Middle initials count. Addresses must be current. If the patient moved last month and the prescription says last year’s address, that’s a red flag.
- Drug name and strength - Generic or brand? Both must be clear. If it says "hydrocodone 10mg" but the label says "hydrocodone 5mg," stop. Double-check.
- Dosage form - Tablet? Capsule? Liquid? Extended-release? If the form doesn’t match the prescribing standard (e.g., a 30-day supply of extended-release tablets for acute pain), dig deeper.
- Quantity prescribed - This is where most errors happen. The number must match the written word. "Thirty (30) tablets" - not "30 tablets." If it’s handwritten and unclear? Call the prescriber. No exceptions.
- Directions for use (sig) - "Take one by mouth every 6 hours as needed for pain" is clear. "Take q6h PRN"? That’s acceptable. "Take 2 tabs bid"? That’s vague. If the sig is ambiguous, you’re legally required to clarify.
Pharmacists who skip even one of these checks risk license suspension. The DEA doesn’t care if you "thought it looked fine." They care if it was verified.
Verifying the DEA Number: The 3-Step Math
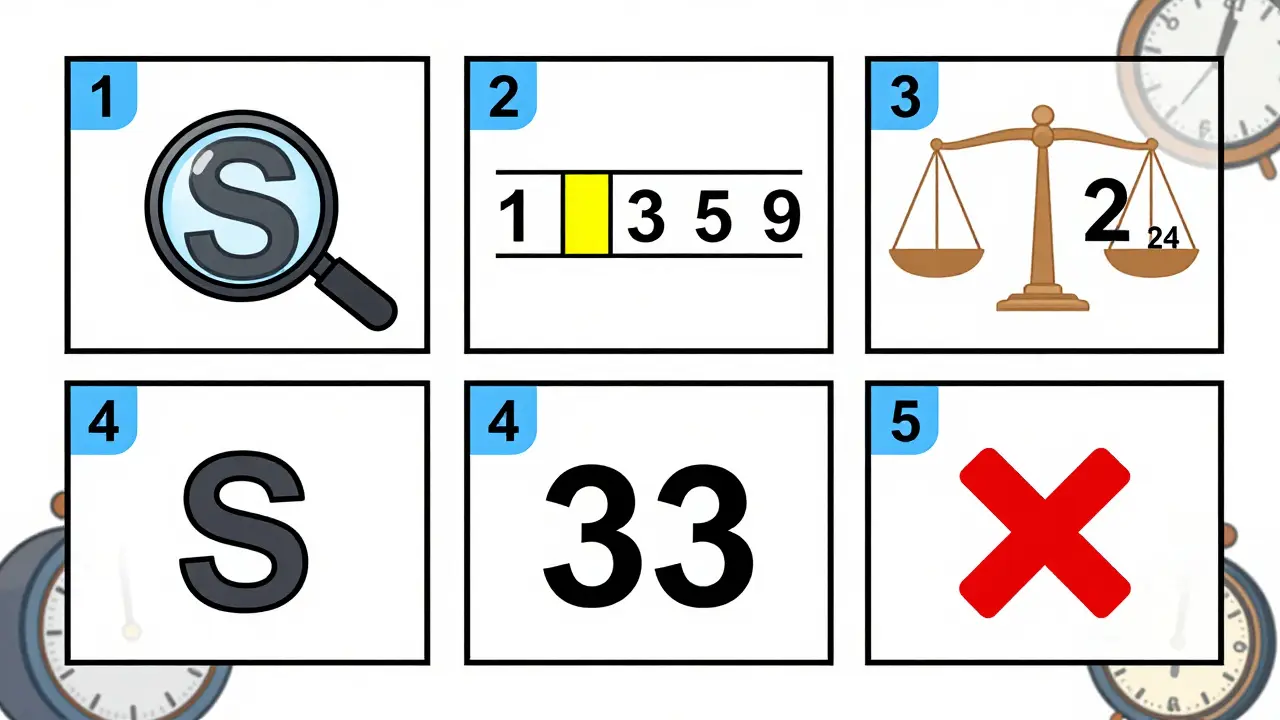
A DEA number isn’t just a random string. It’s a coded identifier with a built-in validation system. The DEA reports this method catches 98.7% of fake numbers. Here’s how to do it:- Check the second letter - It must match the prescriber’s last name initial. If the prescriber is Dr. Smith, the DEA number must be A
1234567. If it’s A1234567, it’s invalid.
- Add the 1st, 3rd, and 5th digits - For example: AB1234567 → 1 + 3 + 5 = 9
- Add the 2nd, 4th, and 6th digits, then double the sum - 2 + 4 + 6 = 12 → 12 × 2 = 24
- Add both results - 9 + 24 = 33
- Compare the last digit - The last digit of the total (3) must match the 7th digit of the DEA number (7 in AB1234567). 3 ≠ 7 → Invalid.
Do this in under 15 seconds. If it doesn’t add up, don’t fill it. Call the prescriber. Document the call. You’ve just prevented a violation.
Quantity Verification: The Hidden Trap
The most common error isn’t a fake DEA number. It’s a mismatch between the numerical quantity and the written quantity. CMS data shows 2% of Medicaid prescriptions were rejected in 2022 because of this. That’s 1 in 50 prescriptions.Example: A prescription says "20 tablets" but the prescriber wrote "twenty (15) tablets." That’s a red flag. The written word overrides the number. If they’re different, you must verify with the prescriber.
For opioids, the quantity must also make clinical sense. The CDC’s 2022 guidelines give conversion factors to compare doses across drugs:
- Codeine: 0.15
- Fentanyl transdermal: 2.4 mcg/hr
- Hydrocodone: 1
- Hydromorphone: 4
- Methadone: 4 (for 0-20 mg/day), 8 (21-40 mg/day), 10 (41-60 mg/day), 12 (≥61 mg/day)
Let’s say a patient gets 30 mg of hydrocodone per day (30 × 1 = 30). The next week, they get 8 mg of hydromorphone (8 × 4 = 32). That’s roughly equivalent. Safe.
But if they get 10 mg of methadone daily (10 × 8 = 80) and 15 mg of hydrocodone (15 × 1 = 15), that’s a 5-fold increase. That’s a red flag. Did the prescriber mean to increase the dose? Or is this a mistake? Verify.
PDMP: The Real-Time Lifeline (and Its Flaws)
All 49 states require pharmacists to check the Prescription Drug Monitoring Program (PDMP) before dispensing controlled substances. But not all PDMPs are created equal.Only 27 states require real-time data (submitted within 5 minutes). The other 22? Some allow 24 hours. A few still let prescribers upload weekly. That’s dangerous.
In 2022, the DEA identified 1,247 cases where delayed PDMP data led to inappropriate prescribing. A patient could get a refill from two different pharmacies in one day, and the system wouldn’t catch it because the last entry was from three days ago.
Use the NABP’s PMP InterConnect platform. It’s the most reliable cross-state tool. Pharmacists who use it report a 37% reduction in verification time. But even with the best tool, you still need to look at the data. Don’t just click "Approved." Read the history. Look for patterns: multiple prescribers, early refills, high doses.
Electronic vs. Manual: Which Is Better?
In 2023, 98% of chain pharmacies used electronic verification systems. Independent pharmacies? Only 58% did. Why? Cost. But here’s the truth: manual verification has an 18.7% error rate. Electronic systems? 99.2% accurate.Here’s the breakdown:
| Method | Accuracy | Cost | Time per Prescription | Compliance Rate |
|---|---|---|---|---|
| Manual Verification | 81.3% | $0 (labor only) | 7.2 minutes | 48% |
| Electronic System (DSCSA-compliant) | 99.2% | $15,000-$50,000 | 3.1 minutes | 91% |
| PDMP-Only | 89% (varies by state) | $0-$5,000 | 5.8 minutes | 73% |
By November 27, 2023, the FDA mandated that all pharmacies use DSCSA-compliant systems. If you haven’t upgraded, you’re already non-compliant. The DEA has started inspections. Non-compliant pharmacies had 31% more diversion incidents than compliant ones.
The 5-Point Verification Protocol
The American Society of Health-System Pharmacists (ASHP) recommends this checklist. Use it every time.- DEA number validation - Do the math. Confirm the second letter.
- PDMP review - Check for recent prescriptions, dose spikes, prescriber changes.
- Prescription integrity check - Look for security paper, microprinting, tamper-evident features. Since 2008, all controlled substance prescriptions must use special paper. If it’s printed on regular paper? That’s a red flag.
- Direct prescriber contact - If anything is unclear, call. Don’t guess. Use the number on file. Not the one on the prescription.
- Clinical appropriateness - Does the dose make sense? Is the quantity excessive? Use CDC conversion factors. If it doesn’t add up, say no.
Dr. John Overstreet, former DEA Diversion Control Director, says: "Single-point verification is insufficient." You need all five. Skipping one isn’t a shortcut-it’s a risk.
What You’re Seeing Today: The Future Is Here
By 2026, every controlled substance prescription will require a QR code linked to a unique product identifier. This isn’t science fiction. It’s federal law under the Drug Supply Chain Security Act (DSCSA). The system will trace every pill from manufacturer to patient.Some states are already ahead. New York’s I-STOP system cut inappropriate opioid prescribing by 75% between 2013 and 2022. California’s CURES 2.0 now talks directly to EHRs, cutting verification time by a third.
And it’s getting smarter. The DEA is launching AI-assisted pattern recognition in 12 states in late 2024. It will flag prescriptions that match known fraud patterns: same prescriber, same patient, same pharmacy, same dose-repeated weekly.
You won’t be replaced by AI. But you will be held to a higher standard. If you’re still relying on handwritten notes and memory, you’re already behind.

Real Stories From the Front Lines
A Reddit user, u/HospitalRPh2020, wrote: "I spent 20 minutes on a methadone script because the quantity was 120 mg, but the sig said 30 mg daily. The prescriber had used the wrong conversion factor. If I hadn’t caught it, the patient would’ve gotten four times their safe dose. I called the doctor. They thanked me. Then they changed their prescribing habits. That’s why we do this."Another pharmacist in Ohio recalled filling a Schedule II script with "200 tablets" written out but "20" as the number. The prescriber had typed it on a tablet and missed a zero. The patient was an elderly woman with chronic pain. If the pharmacist hadn’t noticed? That’s 180 extra pills in circulation.
These aren’t rare. They happen daily.
What Happens If You Get It Wrong?
The penalties are real:- License revocation - One violation can end your career.
- Civil penalties - Up to $758,574 per violation in 2023.
- Criminal prosecution - If diversion leads to overdose or death, you could face federal charges.
DEA inspections in 2022 found 38% of pharmacies had verification deficiencies. Independent pharmacies? 52% failed. Chain pharmacies? 29%. The difference? Systems. Training. Accountability.
You don’t need to be perfect. But you must be consistent. Every time. No exceptions.
Final Checklist: Before You Dispense
Use this before you hand over any controlled substance:- ✅ Prescriber name and address match DEA registration
- ✅ Date is current (Schedule II) or within 6 months (III-V)
- ✅ Patient name and address are complete and current
- ✅ Drug name, strength, and form are correct
- ✅ Quantity: number matches written word
- ✅ Directions are clear and clinically appropriate
- ✅ DEA number passes the 3-step math
- ✅ PDMP shows no red flags (early refills, multiple prescribers)
- ✅ Prescription has tamper-resistant features
- ✅ Clinical dose matches CDC conversion factors
If any box is unchecked? Stop. Call the prescriber. Document the call. Do not dispense.
What if the prescription has a handwritten sig that’s hard to read?
Never guess. Call the prescriber directly using the number on file, not the one on the prescription. Document the time, date, name of the person you spoke to, and what was clarified. This protects you legally.
Can I fill a Schedule II prescription without a DEA number?
No. A valid DEA number is mandatory for all Schedule II-V prescriptions. If the DEA number is missing, illegible, or doesn’t validate, the prescription is invalid. You must return it to the prescriber.
Is it okay to accept a faxed controlled substance prescription?
Yes, but only if it’s a true copy (original signed by the prescriber, then faxed). Electronic prescriptions are preferred. Paper faxes are acceptable under DEA rules, but you must still verify all seven elements and check the PDMP.
Why do some states have different PDMP rules?
Each state runs its own PDMP. Federal law sets minimum standards, but states can add stricter rules. For example, California requires prescribers to check the PDMP before writing a script. New York requires real-time reporting. Always follow your state’s rules-even if they’re stricter than federal ones.
What should I do if a patient says they lost their prescription?
Do not refill a lost Schedule II prescription. Schedule II drugs cannot be refilled under any circumstances. For Schedules III-V, you may refill if the prescriber confirms the loss and provides a new prescription. Always verify the new prescription through all seven elements and check the PDMP for recent activity.
Verification isn’t a chore. It’s your shield. Every time you catch a mistake, you’re not just following rules-you’re saving lives.




